In the coming weeks, The Imprint will feature a five-part series on Fetal Alcohol Spectrum Disorders from Helen Ramaglia, an advocate for foster youth and a member of our Blogger Co-Op.
Part 1 – What Is A Fetal Alcohol Spectrum Disorder?
Fetal Alcohol Spectrum Disorders (FASD) is an umbrella term describing the range of effects that can occur in an individual whose mother drank alcohol during pregnancy. These effects may include physical, mental, behavioral, and learning disabilities with possible lifelong implications.
FASD is the leading known cause of mental retardation in America today. The annual cost to the U.S. of Fetal Alcohol Syndrome alone in direct and indirect cost is approximately $5.4 billion dollars, according to the Minnesota Organization on Fetal Alcohol Syndrome (MOFAS).
The term FASD is not intended for use as a clinical diagnosis. An individual would not receive a diagnosis of FASD. Diagnoses like Fetal Alcohol Syndrome (FAS), partial Fetal Alcohol Syndrome (pFAS) and Alcohol-Related Birth Defects (ARBD) fall under the umbrella of FASD.

http://www.mofas.org/
Children and adults who suffer from these disorders frequently exhibit other physical and behavioral challenges. According to MOFAS:
• 90% of individual with an FASD also have a mental illness
• 50% of adolescents and adults displayed inappropriate sexual behavior
• 60% of people with an FASD have a history of trouble with the law. The average age children with FASD start getting in trouble with the law is 12.8 years old.
• 50% of individuals with an FASD have a history of confinement in jail, prison, residential drug treatment facility, or psychiatric hospital.
• 80% of children with an FASD are not primarily raised by a biological parent
• 70% of children in foster care are affected by some type of prenatal alcohol exposure
• 60% of adolescents with an FASD experienced significant school disruptions
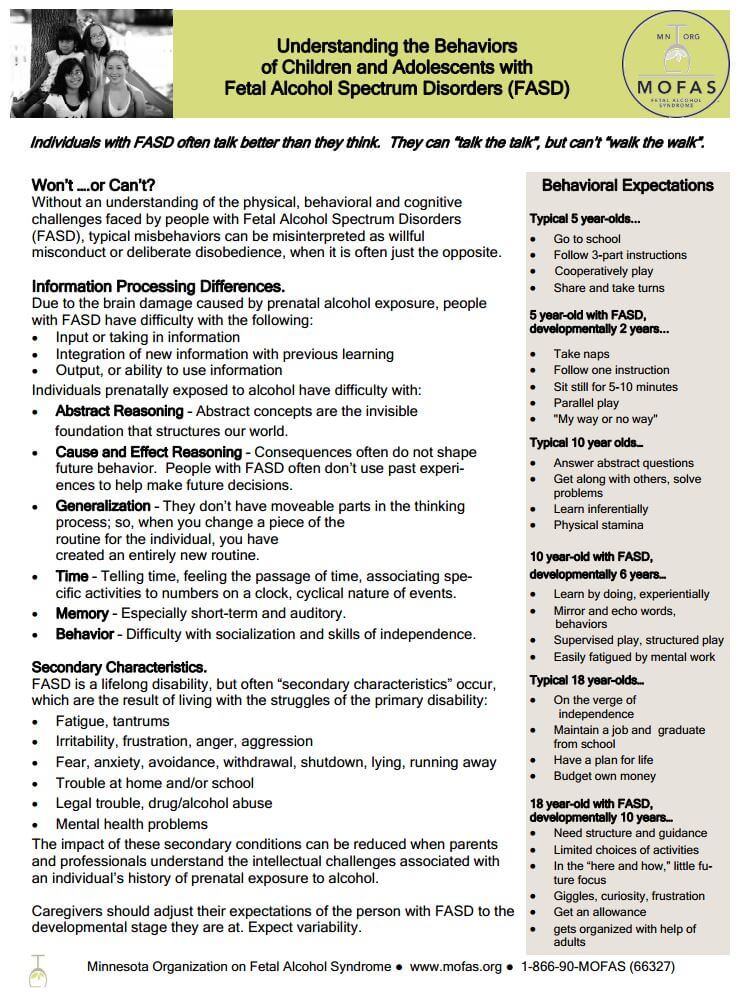
Without an understanding of the physical, behavioral and cognitive challenges faced by people with FASD, typical misbehaviors can be misinterpreted as willful misconduct or deliberate disobedience, when it is often just the opposite.
There are many behavioral characteristics which differentiate FASD patients with other individuals suffering others forms of mental disabilities. Some examples, from a fact sheet compiled by the Texas Department of Family and Protective Services:
- Individuals with FASD often speak better than they think. Socially, they tend to be very outgoing and socially engaging, yet they are frequently seen by others as intrusive, overly talkative, and generally unaware of social cues and conventions.
- Poor social judgment and poor socialization skills are common, and many patients are hungry for attention, even if it is negative. Due to their social immaturity, they have difficulty establishing friendships, especially with children of the same age.
- Children with FASD frequently have learning difficulties. These difficulties result from poor thinking and processing skills. Information may be known, but cannot be applied to different situations. Learning may occur in spurts. Easy learning periods may be followed by harder ones.
- During difficult periods, children may have trouble remembering and using their learned information. Because of inconsistent learning, teachers may think they are just not trying. They may label them as lazy or stubborn.
Caregivers should adjust their expectations of behaviors of the person with FASD to the developmental stage they are at. A five-year-old with FASD is often times developmentally on par with a 2-year-old; a 10-year-old is on par with a 6 year-old; and an 18-year-old is on par with a 10-year-old.
www.mofas.org
Parents may be able to mitigate some of these behavioral issues by establishing daily routines and using clear concise language and examples, teaching skills for daily living, and rewarding children to reinforce good behavior. For older youths with a FASD, vocational training and social skills training may be helpful.
Because symptoms and abilities can vary, each person should be assessed individually to determine the best combination of interventions. In addition, people with an FASD are at greater risk for developing substance abuse problems.
Check back soon for Part 2: The Financial Impact of FASD
Helen Ramaglia is a foster alumni who became a foster/adoptive parent. She is the founder and Director of Fostering Superstars, a Congressional Award Winner for her work with foster children and is the author of “From Foster to Fabulous”. She is a popular speaker, trainer and advocate for foster children.
Want to share your opinion or analysis with colleagues in the youth services field? Join our one-of-a-kind Blogger Co-Op, and share in the benefits from your work!
Other Resources on FADS:
• Centers for Disease Control & Prevention: http://www.cdc.gov/ncbddd/fasd/index.html
• Fetal Alcohol Disorders Society: http://www.faslink.org
• Nemours Foundation (Spanish): http://kidshealth.org/parent/en_espanol/embarazo/fas_esp.html
Links to more information on FADS:
http://depts.washington.edu/fasdpn/htmls/fasd-fas.htm
https://www.mofas.org/fasd/criminaljustice
http://www.arcnc.org/fetal-alcohol-syndrome
http://www.mayoclinic.com/health/fetal-alcohol-syndrome/DS00184/DSECTION=symptoms
http://www.dfps.state.tx.us/Adoption_and_Foster_Care/About_Our_Children/Disabilities/fetal_alcohol.asp


