Proposed legislation, and the prospect of yet another class-action lawsuit against the state, may press lawmakers to resolve the issues preventing kids placed in out-of-county foster homes from getting needed mental health treatment.
Thousands of California foster youth who have been placed outside their home counties are entitled to mental health services, but may not receive them due to a classic case of bureaucratic hot potato.
A bill to fix this, Assembly Bill 1299, unanimously passed the Assembly in June and will be heard in the California Senate Health Services Committee on July 14.
AB 1299, which was introduced by State Assemblyman Sebastian Ridley-Thomas (D), would require the California Department of Health Care Services (DHCS) to create clear policies to guide the transfer of responsibility for mental health services to a child’s county of residence. The bill would also compel the Department of Finance to establish a system to ensure that counties are fully reimbursed for providing mental health services, during the fiscal year when the services are delivered, by May of 2016.
All California foster youth are eligible for Medi-Cal, the state’s public health insurance program. But under current law, when a foster youth moves to a different county, responsibility for providing mental health services—and any related funding—remains with the county of origin and its network of service providers
As a result, nearly 12,000 out-of-county foster youth—or about one in five of all youth in the state’s child welfare system—are routinely left in limbo, waiting for mental health services that often take months to begin.
A 2011 report from the state’s Child Welfare Council, which is responsible for improving collaboration among child-serving agencies, revealed disparities between children in and out of county who were receiving mental health services. An examination of the data for all 58 counties in California showed that out-of-county youth received fewer average days of mental health outpatient or day services when compared to children with in-county placements (2.3 days versus 2.9).
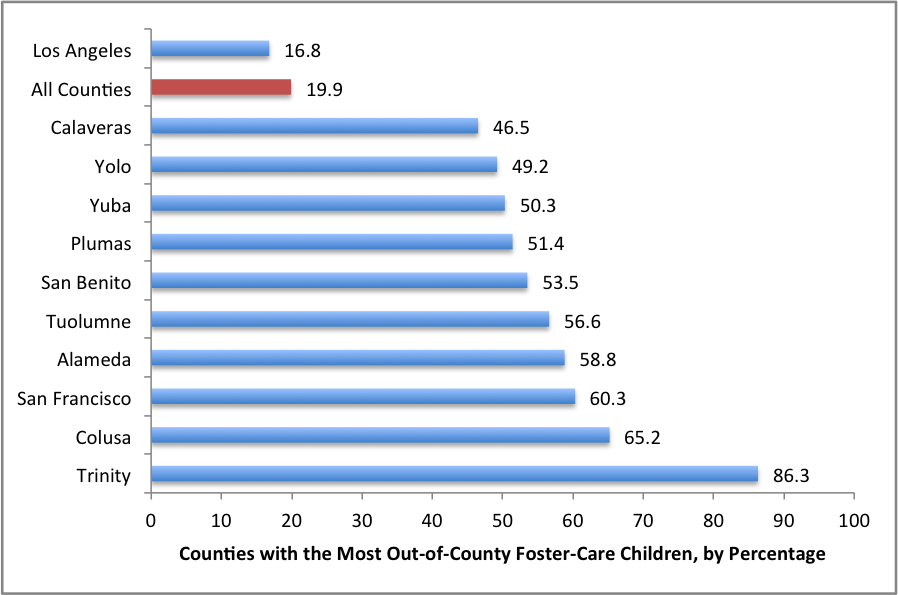
The percentages represent the number of foster children from each California county who are sent to another county or out of state. “All Counties” is the average of all 58 counties. This data was pulled from a count of foster care placements in California on January 1, 2015, from CWS/CMS accessed through the University of California-Berkeley’s California Child Welfare Indicators Project.
“Part of the issue is that the counties have been in control of the money up until this point, and the money has not been flowing as it needs to when these kids are moving from one county to another,” said Khaim Morton, chief of staff for Ridley-Thomas. “We want to get to the point where we can collaborate and reach a compromise that will enable more of the money to reach these kids and more swiftly.”
California may once again find itself back in court as part of a class-action lawsuit if there isn’t an agreement soon, according to mental health advocate Patrick Gardner, founder of Young Minds Advocacy Project.
“If there isn’t a solution by the end of the year, either through negotiations under the auspices of the Child Welfare Council or through the work being done in the legislature, a judge is going to have to step in to fix this, because letting this continue is completely unacceptable,” said Gardner.
A lack of coordination between child welfare and mental health systems throughout the state has long made the collaboration needed to serve out-of-county youth difficult, a point acknowledged by DHCS in a memo that outlines the state’s goals in providing a fix.
“The highly confidential nature of personal/medical information concerning foster youth has made it challenging to coordinate services among all of the government agencies that are involved in their care,” DHCS Information Officer Carol Sloan wrote in an email to The Imprint.
A recent data-sharing agreement between DHCS, the Department of Social Services and counties will enable the exchange of confidential data, and DHCS hopes this will speed up the delivery of mental health services to out-of-county foster youth.
The state has a roadmap of sorts for partnerships on mental health and foster care in the 2011 Katie A. v. Bonta decision, which resolved a federal class-action lawsuit filed on behalf of California foster youth and children at risk of out-of-home placement who had been chronically denied mental health services.
“Mental health and child welfare need to be brought together to solve these problems,” said Richard Saletta, who served as special master in the state’s court-monitored Katie A. settlement. “Some of these problems that the legislature is trying to address now—via medication or via out-of-county placement issues—these issues could be resolved if there were some agreements around shared responsibility for outcomes for these kids. That’s what Katie A. offered—how to bring child welfare and mental health together.”
One layer of complexity will be defining the types of exemptions that county administrators may claim under the proposed policies for transferring responsibility for out-of-county foster youth. Some of these youth may benefit from continuing mental health services in their county of origin in certain situations.
But without a clearer set of protocols—much like the processes used to offer healthcare to out-of-county foster youth—Gardner said thousands of these youth will continue to miss out on the services they need.
“My concern is that a lot of the proposals washing around are essentially the exceptions swallowing up the rule and will continue to have the same approach as what’s happening now,” Gardner said. “If you don’t have a systems response, you’re not going to solve the problem. You’re just going to add complexity. When you add complexity, you make it more difficult to access services, and the general outcome is that the status quo remains.”



